
This May 1977 abortion-rights march (which numbered about 300) – seen here in Parliament grounds – was probably prompted by the Commission of Inquiry into Contraception, Sterilisation and Abortion, set up by the government to deal with the perennially controversial topic of abortion. Many of the marchers were young members of the Women’s National Abortion Action Campaign, accompanied by a sprinkling of male supporters. Although abortion was largely seen as a women’s issue, it also concerned many men. Some wanted their wives or girlfriends to have access to it, while others were fiercely opposed.
In 1978 Members of the Women's Electoral Lobby (WEL) protested in Nelson with the signs "Abortion a Woman's Right to Choose" and "Not the church and not the state, women must decide our fate". The women are wearing chains to symbolise the restrictions suffered by the women who are unable to access abortions.
In 1978 Members of the Women's Electoral Lobby (WEL) protested in Nelson with the signs "Abortion a Woman's Right to Choose" and "Not the church and not the state, women must decide our fate". The women are wearing chains to symbolise the restrictions suffered by the women who are unable to access abortions.
The defining issue of the Second Wave of Feminism was its support fro abortion as a matter of choice for women and their doctors. It was essential for most women in the 1970’s to control their fertility. Abortion was often used as a method of birth control; there was no knowledge of contraception if women did become pregnant home remedies were sought. Economic hardship and a desire to provide the best for children already born encouraged women to limit the number of children and space their pregnancies. A single women who became pregnant was in truly desperate circumstances. A woman columnist wrote in 1944 “If you know the cruelty of women to the Magdalenes of this world! A thief may be caught and sent to prison for his crime; when he is free he has a chance to begin afresh, and decent people will want to help him. But the unmarried mother is branded all her life as a criminal against society”. In the early stages of pregnancy women jumped from tables and threw themselves downstairs to bring on a late period. Chemists readily sold a variety of substances reputed to cause miscarriage. Many of these were advertised ambiguously as cures for “female irregularities” or to “remove obstructions”. Slippery seaweed tents were also used, which when inserted in the cervix, expanded with moisture from the body and could induce a miscarriage. Women also used what was hand such as alcohol, laxatives and Epsom salts, all of which would have been useless. Women also used knitting needles and other household items; with one women who inserted caustic soda and was “eaten away”. However the surest way to perform an abortion successfully was by visiting a professional. The underground abortion industry flourished, driving women to desperate measures. Women who did not have the necessary money or contacts for an professional abortion visited “backstreet” abortionists who varied in their methods, skills and prices. Abortions were performed any where from hotels to private homes, with some setting up small hospitals. Skilled operators made a lot of money.
During the 1950’s and 1960’s the number of abortions performed in hospitals on psychiatric grounds had increased by the process of seeking an abortion was often humiliating with women having to present their case to a panel of usually male specialists. Women who went to backstreet abortionists in the early 1960’s and between 200-300 women were admitted to hospital each year following illegal abortions. Abortion was the agenda of the Women’s Liberation Movement from the beginning. Some groups referred women to skilled back street abortionists or put together menstrual extraction kit, a method of self performed abortions copied from American feminist heath clinics. In April 1972, the first national women’s liberation conference adopted the demand for “A women’s right to choose” and in 1973 the Women’s National Abortion Action Campaign (WONACC) was launched. It took the uncompromising stance of the repeal of all abortion laws. Christine Dann commented, “The Women’s Liberation Movement did not beg, plead, or pussyfoot around. It demanded a safe and open right to something women had traditionally obtained with guilt, shame, secrecy and danger. Other key groups in the campaign for abortion was the Abortion Law Reform Association of New Zealand (ALRANZ), established in 1971 to counteract the activities of the main anti-abortion group, the Society for the Protection of the Unborn Child (SPUC). ALRANZ hoped to prude public opinion of the law. ALRANZ National President Isabel Stanton said “We do not see abortion as purely women’s rights issue, we see it as a question of responsible reproduction and parenthood. We hate the phrase “abortion of demand”’. In May 1974 New Zealand’s first abortion clinic, the Auckland Medical Aid Centre (AMAC) opened its doors. On 17 May 1974, in a refitted residential house in Remuera, the Auckland Medical Aid Trust opened New Zealand’s first abortion clinic. For $80 it provided women who met the legal criteria with counseling and pregnancy termination. The clinic represented change for women, as well as for their doctors, who offered support. It used the latest vacuum aspiration technique, provided counseling, and planned to operate within the law as it then stood. AMAC was opened by a group of ALRANZ supported, including Isabel Santon.
Women flooded in from all over New Zealand to get abortions. The Women’s Liberation Movement provided many of the AMAC staff. Tony Church, who had convened the first United Women’s Convention was the manager. There was immediate controversy. By September of 1974 Broadsheet was predicting that the question of the abortion clinic “seems to be developing into a full scale political hot potato. It predicted police action or legislation. In mid- September based on acomplain by a SPUC member the Auckland police made an illegal raid on the clinic. The police photographed rooms and equipment, inspected rubbish being burned in an incinerator by a nurse, and took hundreds of confidential patient files to search for illegal abortions. Doctors were outraged and hundreds of people took part in rallied outside the Auckland Central Police Station and Parliament Buildings. As a result of the raid the clinic’s operating doctor, Dr James Woolnough, was charged on twelve counts of procuring illegal abortions, but after three trials he was eventually acquitted. At the same time AMAC supporters were trying to influence MPs not to vote for a private member’s Bill introduced by Dr Gerald Wall. It required that all abortions be performed in licensed hospitals. Petitions were signs, and contingents of women all around New Zealand were bused into Wellington for the second reading of the Bill to demonstrate women’s opposition. However MP’s expressed views that showed how conservative they were on the subject. When the Bill went through, AMAC was forced to shift into a private hospital, but the abortions went on. Anti- abortion protestors increased their efforts, staff and clients had to contend with a three-month long “vigil” outside the hospital’s front gates. When protestors chanted around a cross, and even thumped wooden-sticks on a miniature coffin, the women in the operating theatre heard the sounds. Then in 1976 the hospital suffered $100,000 damage in an arson attack, but it still did not close. In just a few years abortion went from being a shameful secret to an urgent national issue. For feminists it was the major focus of the 1970’s. politicians and professional organisations which had conveniently ignored it for decades were forced to make a public stand. In 1975 the National Government appointed the Royal Commission of Inquiry into Contraception, Sterilisation and Abortion to examine the whole question. After months of hearing submissions that the majority of New Zealanders believed that abortion should be a matter between a woman and her doctor. Instead its report, which was finally released in April 1977, recommended the establishment of medical panels to whom women must present their case. The only organization that supported the change was SPUC; it was opposed by dozens of medical professionals and women’s organisations. These groups formed coalitions, which had the formidable task of translating the weight of the public and professional opinion against the Contraception, Sterilisation and Abortion Bill into effective action. Years of supplying reasoned information had not noticeably changed MP’s opinions on abortion. Over the next few month amendments were introduced turning the Bill, which had never been a liberal document, into one of the most restrictive pieces of abortion legislation in the Western world. It required women to out their case to two approved doctors called “certifying consultants”. In Wellington pro-abortion activity was centered on MP Marilyn Waring’s office. People sat or lay in the corridor throughout the night during the final debate. Their mood turned from “mid unease to sheer horror” as the implications of the legislation was being passed. One of the amendments stated that abortion would only be legal if the danger to the women’s health “could not be averted by any other means”. AMAC doctors refused to work under such an ambigyous provision, and the clinic closed with one days notice. Joss Shawyer, wo had worked as a counselor, immediately approached the Broadsheet Collective to publicise a new organisation she was founding called Sisters Overseas Service (SOS) to help women fly to Australia. Stickers were pasted across the front of the January issue of Broadsheet which had already gone to the press saying “where to get an abortion- see inside” and leaflets about SOS were tucked into every copy. Women in the 1970’s simply were not prepared to go back to the days of dangerous illegal abortions, no matter what the government said. SOS told the Abortion Supervisory Committee in July 1978 that over seven months it had referred 1,000 women to abortion clinics in Sydney. “This involved an overall cost of half a million dollars. 352,000 was spent on air-fares, the government reaped $32,000 in travel tax and $2000 in airport departure tax and the Sydney clinics netted $100,000”. Braches of SOS were set up around the country and by 1979 the Auckland office had expanded into a full-time service. In February 1978 a petition was launched calling for the repeal of the Contraception, Sterilisation and Abortion Act. The idea was formed by women in influential positions but eventually it involved hundreds of ordinary women, working from 28 branches, who collected signatures throughout New Zealand. It carried 318,820 signatures, each one checked against the electrol roll, making it New Zealand’s biggest petition gathered in the shortest time, and the third biggest petition overall. It was therefore a brutal disappointment when the petition was given a low rating for consideration by the Petitions Committee, preventing it from being formally presented to Parliament. Eventually the Parliament could not ignore urgent requests from its own advisory body on abortion, the Abortion Supervisory Committee (ASC), which had been set up to administer the new legislation. The ASC requested crucial changes to make the law workable. In the wake of unrelenting criticism the ASC also had to modify its interpretation of the law to ensure that there were sufficient certifying consultants and abortion facilities to provide a service within New Zealand. In August 1979, after frustrating delays, AMAC was finally granted a license and reopened. Public abortion services were also established in Auckland and Wellington. In 1981, the ASC reported that the “Australian traffic” had almost ceased with most abortion to New Zealand women taking place in New Zealand. In the following months that followed, the number of legal abortions performed in New Zealand fell by more than 50%, dropping from nearly 6,000 in the year to March 1977 to just over 2,600 in 1978. Eighteen months after the passage of the new abortion legislation in New Zealand, Marilyn Pryor wrote in 1979 “it would appear that the abortion juggernaut has been constrained and there is some hope that the time may be turning back.” Abortion became accessible for most women, and safer than a decade before, abortion services remained unevenly available, and South Island women continued to make an expensive and stressful trip to Auckland in the 1990’s. Now abortions are easily available, for every female in New Zealand. In the end, there is a clear answer to every challenge and obstacle put forward by those trying to restrict women’s reproductive freedom. Dr. George Tiller says “trust women”.
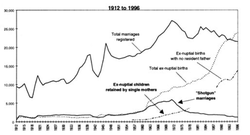
Access to abortion was a long term significance of the Second Wave of Feminism for New Zealanders. (Shown in the top photo) The statistic shown by Statistics New Zealand shows in 1961 births were at a high, slightly lowered in mid 1960s, this could be due to backstreet abortionists. In 1970 it started to rise, but after 1971 it had a dramatic drop from 64,000 births to 50,000 births in 1981. This reflects the legalization of abortion in December 1977. Legalizing abortion has become a very significant event in New Zealand; feminists believed abortions would be a last resort. However the abortion figures were not anticipated or that abortions would become a backstop contraceptive measure for some women. New Zealand’s abortion rate now exceeds Germany, the Neverlands and Finland. Contraception is now freely available to even underage children, and sex education starts at primary school. But the number of 11 to 14-year-old girls having abortions has increased 144% in the past 15 years, and among 15 to 19-year-olds by 74%. Teenage pregnancies make up nearly 25% of all abortions. For every teenager who gives birth now, another has an abortion, and one in four pregnancies of women of all ages currently ends that way. A 1936 investigation in this country guessed that one in five New Zealand pregnancies ended in abortion then at a time when abortion was legal only to save the mother's life. In the past 30 years, the number of abortions performed annually has soared from 4682 in 1976 to 17,934 last year.
http://www.teara.govt.nz/en/speech/29023/abortion-rights-march
This is a video relating to the abortion debate in the 1970's. Abortion marches became more common and widely talked about in New Zealand society. This video shows a abortion march in 1973 including arguments against and for abortion.
All of this information is accurate and true, most of my information came from a thesis by Hayley Marina Brown who did a strong and detailed thesis on the Advocacy of Abortion Law Reform in New Zealand and New South Wales from the 1970s. I felt that all the information was really well presented on Te Ara Encylopedia of New Zealand which provided my primary material.
http://ir.canterbury.ac.nz/bitstream/10092/948/1/thesis_fulltext.pdf
Joan’s Story
Joan wrote her story after seeing my letter in the Listener
My abortion took place in 1970. I have always loved babies. In fact, I started wanting one of my own when I was only about 11 years old. When I was 21 I met Sam, the love of my life. Unfortunately, he was also the love of someone else’s life – his Wife’s! He eventually left his wife, and we have been together now for 35 years and have four grown-up children.
About six months after we met, I became pregnant. First off, I was absolutely thrilled, at least for myself. Sam wasn’t too happy about it as he was not yet divorced. When I got over the euphoria of the thought of having a baby, I started to think in a more practical manner. First, I had not met Sam’s family, second I had no money, and third he didn’t have much either. Oddly enough, the one thing that made me start thinking of abortion was the fact that I could not have afforded to buy my child-to-be a tricycle of all things! I knew Sam would eventually get married. So we agreed I would have an abortion and do things in the right order.
First, get your abortion. I had heard of a doctor who was purported to help girls ‘in trouble’ so I went to see him. He confirmed the pregnancy, and I was to see him (memory a bit hazy here) every day for three or four days to take tablets that might bring on a miscarriage. But they didn’t work. he then made arrangements for me to have an abortion in Sydney.
Sam and I flew to Sydney on a Thursday, and I had the abortion on a Friday. The rooms were every bit as bad as I had imagined, filthy concrete stops leading up to a hold in the wall. The nurse was very kind. As I was in tears she made sure I really did want to go ahead with it. Afterwards, I was given the most painful penicillin injection, which I can fee to this day.
We stayed in Sydney for a couple of days and arrived back on the Sunday. That night I was bleeding and in awful lot of pain so I rang the doctor who was obviously entertaining friends and he told me to take a painkiller and go to bed. When I went to see him next, he made what I thought were unprofessional comments and asked me questions like, ‘When do you and your boyfriend have sex? In the morning? At night?’
Then it was time for an internal examination. Let me tell you I had to keep my brain firmly in neutral and concentrate on a spot on the wall or I would have had an orgasm, as he stimulated my clitoris. Some years later this doctor was charged with (I think) indecent assault, and I can remember saying to Sam, ‘I bet she had had an abortion too!’ It was such a shameful secret you wouldn’t want anyone to know, and the doctor had that over you.
I think the worst thing about abortions in those days was the shame and the secrecy. I couldn’t tell anyone, and the guilt was something I could only share with Sam. Contrast that to the way sex (or unmarried sex) is so out in the open these days. Some years ago I was at the gynaecologist’s room with my daughter and her boyfriend as the four of us discussed her contraception. It wouldn’t have happened back then.
Joan's story is touching but because of confidentiality the reader can't guarantee that the story is genuine; it could be exaggerated, false, or misrepresented. However, throughout the book and within other literature there are anonomous stories to the same extent. The book was made to tell the true stories of the women who had abortions; I believe that Sparrow would have done research before publishing the story to ensure it was true. The story is very accurate to the overall feel of abortions at that time; such as the shame and secrecy.
John Taylor’s Story
Mr John Taylor (1928-2008), consultant obstetrician and gynaecologist of Auckland, died on 30 December 2008. He was a key provider of services in Auckland for many years and was a respected teacher and trainer. He was interviewed in 2006.
The specialist I mostly worked with taught me a lot of obstetrics, which as a young GP I appreciated. He was great. He would come out any time I had a problem when a more experienced person may not have needed to call upon him. At the end of it he said, ‘You know you’re really enjoying this aren’t you?’ I said, ‘I have to be absolutely honest, yes I am’. He said, ‘Have you ever thought of going into O&G?’ I said, ‘I really have enjoyed this year and the training you’ve given me’. ‘Well, look’, he said ‘would you be interested in doing six months as a registrar in St Helen’s Hospital in Christchurch? You’d be working with some very fine people down there’. And I said, ‘Yes I think I would be interested. I think I could do that’.
So I went to Christchurch and I was a registrar at St Helen’s Hospital for six months. It was a wonderful six months. My career plans changed and I decided to go on with O&G. I was appointed as a house surgeon at National Women’s and then as a registrar before going overseas for further specialist training.
While at National Women’s there was one particular case that had a lasting impact on me. In October 1957 a lovely young lady was admitted to National Women’s Hospital where I was the registrar in the ‘C’ Team. She had been languishing in bed getting more and more ill, and came in with a high temperature of about 104 degrees. She had been too scared to present to anybody for medical help. As it transpired she had been to an illegal abortionist and the uterus had been only partially emptied of a 12 week pregnancy.
She was suffering from severe septicaemia to the extent that she had blood pressure collapse. We first had to attend to that, trying to sustain her blood pressure with noradrenalin drips. For the infection she was given massive doses of antibiotics. She had a lot of abdominal pain but for most of the time remained conscious. It reached the stage where the decision had to be made whether or not she should have a hysterectomy. This would have removed the cause of her septicaemia, the infected tissue in the uterus. However, the specialist in charge decided not to operate because her condition was so poor she would not have survived.
To make a long story short, after we had worked desperately with her for about 10 days, she died. As a team we had put so much time, effort and skill into trying to save her that her death came as a profound loss. I was severely affected by this tragedy, and I think it influenced the rest of my career in O&G.
We knew the social history and the circumstances surround her particular situation and what led to her having an abortion. They were just social pressures but pressures so strong that she felt desperate. Behind it all was the disgrace of having a baby out of wedlock. She couldn’t face up this this and didn’t want to disappoint her relatively conservative parents. We never found out where exactly she had been for the abortion. We left that to the police.
For this lovely young lady to lose her life in this way made me think there must be a better way. The numbers coming in with complications from illegal abortions were not huge. I suppose about one a month. When I say about one a month I’m only referring to one particular team. There were four teams, and they all had their own acute admissions. I didn’t like to pressure any patient so I never found out much about the illegal networks.
I was overseas for a year (1960) and then, having sat the exam in London, I was appointed registrar in the King’s College group of hospitals. I was then invited back to practise in Auckland and subsequently was appointed as a consultant at National Women’s. In my specialist training I learnt about abortion through clinical experience. I was exposed to septic abortion in England and there were other cases that reinforced my view but it was that one unforgettable case back in New Zealand in 1957 that turned it around for me.
With respect to my professional colleagues on the ‘C’ Team at National Women’s I suppose I felt more strongly than they did. Some of the senior consultants believed that if the grounds were mental health then you needed to get a psychiatric opinion to confirm that. That idea never appealed to me. I just thought it was a total farce to engage a fully qualified specialist psychiatrist on an abortion case. Our team only did abortions if there was a physiatrist who could say the women was likely to suffer severe depression.
Women had to go before a penal of three consultants, set up by the hospital to deal with requests for abortion. I remember when I’d only just been appointed as a very junior consultant forming part of a panel with two very senior gynaecologists. The other two said to me, ‘Of course there’s no way this woman will by psychiatrically affected. What do you think?’ and I said,’I just can’t agree with you I’m sorry’. They felt just as strongly as I did but in keeping with their own conservative views. I thought, ‘There’s got to be a better way. This is just untenable’.
At the panel the woman was interviewed in person; it was not just a matter of reading case notes. Consultations with the panel and the woman could take half an hour or so. After the consultation the panel conferred and made their decision. Then the woman wa brought back in to receive the decision in person. As far as my colleagues were concerned it was just open and shut. If she was a woman who was temperamentally normal in every other respect they could see no grounds for termination. At that time I suppose a strict interpretation of the law would be in accordance with their view.
I could ask specifically for a psychiatric report, but some of the psychiatrists were conservative bent, and they would agree with my conservative colleagues. One or two more liberal psychiatrist supported my professionally and would issue a report in favour of my opinion. But in general the whole scene was conservative because none of the senior gynaecologists were liberal at that time.
The ground of fetal abnormality raised different issues. Abortion was acceptable where there was a risk of a baby being born with a serious abnormality. The specialist had the surgical skills to undertake abortions, and I learnt surgical skills from them although I did very few as a registrar.
When I set up my specialist practice I included abortion services as part of women’s health care. It was not subjected to pressure from professional colleagues, even those with strong religious convictions. I always totally understood their situation and they mine. Increasingly colleagues came round to accepting the situation we had come to practise and at no stage did my views on abortion affect my professional development with regard to committees and jobs.
When the law changed, and the Auckland Hospital Board was required to provide an abortion service, I was invited down to a red carpet lunch, with hospital board cars provided, to meet Dr Fred Moody OBE, medical superintendent in chief. He said ‘John I want you to set up an abortion service for the Auckland Hospital Board.’ He had no doubt about wheat he was doing because he knew of my abortion views through my consultant colleagues. He wanted me to set up the Epsom Day Hospital and become its first medical director.
An earlier attempt to establish a day clinic by the Auckland Hospital Board had foundered. A licence was granted in May 1978 to St Margaret’s as part of the public hospital system. The previous owner, a doctor who did deliveries (and allegedly abortions), had left the premises to the Auckland Hospital Board. There was a huge fuss over the name because St Margaret is a Catholic saint who was killed for refusing to have sex with a Roman priest. She did a virgin and a martyr and became a patron saint of pregnant women.
Dr Peter Wilcox who previously worked as an operating doctor at AMAC, was appointed in June 1978, but resigned after his application to become a certifying consultant was refused by the ASC. Dr Wilcox’s case was raised in Parliament in July 1978 during the final debate on the amendments to the CS&A Act.
After my involvement in the Epsom Day hospital became known as SPUC used to protest outside our home when we had young children. It was pretty tough on the kids to have these banners and so on. My car used to be attacked, and graffitied, and tyres let down. They’d put stickers on the front and back windows – ‘Baby Killer’ – and all that kind of thing. One way and another I had quite a lot of contact with the SPUC people. I used to invite them to have a cup of morning tea. Our neighbours weren’t quite so happy. They used to turn the hoses on an inadvertently spray them. I didn’t find protest activity easy to take especially when it affected my wife and family. They kids had to cope at school, but I must say it didn’t stop my daughter studying medicine and becoming involved in abortion services.
I believe the law must allow for termination for a woman who finds herself profoundly desperate with an unplanned and unwanted pregnancy. I realise I may sound old fashioned and not in full accord with ALRANZ’s viewpoint, but I’ve always believed the present law isn’t too bad because it allows for termination on the grounds of mental health. I believe that if a women is forced to continue her unwanted pregnancy, then it is highly likely to adversely affect her psychological health to the extent that her health is endangered.
The present law is workable, and if you can judge things by the end results then it is very safe. There has not been a maternal death directly attributable to abortion since the new laws have been in place although the law cannot take the credit for that. The use of antibiotics to treat septic abortions was the most dramatic and life-saving advance. Furthermore the medical profession’s priority of saving lives as opposed to reporting crimes encouraged women to see medical treatment. The suction method using flexible cannulas was an improvement and could be carried out under local anaesthesia. Improvements in general anaesthesia made that safer when local anaesthesia was not an option. The use of ultrasound made the diagnosis of abnormalities and the estimation of gestational age more accurate. There were also improvements in blood transfusions, other intravenous fluids, and the treatment of pulmonary embolus (a risk after childbirth or abortion when a blood clot travels to the lungs). As well as these medical advances there has also been a general improvement in the nutrition and general health of the population.
The gain was not just in saving women’s lives but in protecting the health of the women. Unsafe abortions did not always kill, but could cause damage to the reproductive organs leaving a woman to suffer from painful complications or infertility, the inability to have children when they wanted to. I am convinced that total control over her fertility is a women’s right.
This story featured in the book Abortion Then and Now, a reliable and recognised book telling abortion stories during the Second Wave of Feminsim. http://alranz.wordpress.com/2013/07/12/history-and-dame-barbara-goodman/ backs up the story featuring in the book, it describes John Taylor and a brief description about his life and his job. As an author Margaret Sparrow, tells other peoples stories as quoted by them. However she has bias; she had an illegal abortion and heard stories later which lead her to write the book. Margaret Sparrow was one of the Family Plannings most well-known doctors, after she attended a Family Planning Association conference she continued to exceed to give women options such as contraception.
Joan wrote her story after seeing my letter in the Listener
My abortion took place in 1970. I have always loved babies. In fact, I started wanting one of my own when I was only about 11 years old. When I was 21 I met Sam, the love of my life. Unfortunately, he was also the love of someone else’s life – his Wife’s! He eventually left his wife, and we have been together now for 35 years and have four grown-up children.
About six months after we met, I became pregnant. First off, I was absolutely thrilled, at least for myself. Sam wasn’t too happy about it as he was not yet divorced. When I got over the euphoria of the thought of having a baby, I started to think in a more practical manner. First, I had not met Sam’s family, second I had no money, and third he didn’t have much either. Oddly enough, the one thing that made me start thinking of abortion was the fact that I could not have afforded to buy my child-to-be a tricycle of all things! I knew Sam would eventually get married. So we agreed I would have an abortion and do things in the right order.
First, get your abortion. I had heard of a doctor who was purported to help girls ‘in trouble’ so I went to see him. He confirmed the pregnancy, and I was to see him (memory a bit hazy here) every day for three or four days to take tablets that might bring on a miscarriage. But they didn’t work. he then made arrangements for me to have an abortion in Sydney.
Sam and I flew to Sydney on a Thursday, and I had the abortion on a Friday. The rooms were every bit as bad as I had imagined, filthy concrete stops leading up to a hold in the wall. The nurse was very kind. As I was in tears she made sure I really did want to go ahead with it. Afterwards, I was given the most painful penicillin injection, which I can fee to this day.
We stayed in Sydney for a couple of days and arrived back on the Sunday. That night I was bleeding and in awful lot of pain so I rang the doctor who was obviously entertaining friends and he told me to take a painkiller and go to bed. When I went to see him next, he made what I thought were unprofessional comments and asked me questions like, ‘When do you and your boyfriend have sex? In the morning? At night?’
Then it was time for an internal examination. Let me tell you I had to keep my brain firmly in neutral and concentrate on a spot on the wall or I would have had an orgasm, as he stimulated my clitoris. Some years later this doctor was charged with (I think) indecent assault, and I can remember saying to Sam, ‘I bet she had had an abortion too!’ It was such a shameful secret you wouldn’t want anyone to know, and the doctor had that over you.
I think the worst thing about abortions in those days was the shame and the secrecy. I couldn’t tell anyone, and the guilt was something I could only share with Sam. Contrast that to the way sex (or unmarried sex) is so out in the open these days. Some years ago I was at the gynaecologist’s room with my daughter and her boyfriend as the four of us discussed her contraception. It wouldn’t have happened back then.
Joan's story is touching but because of confidentiality the reader can't guarantee that the story is genuine; it could be exaggerated, false, or misrepresented. However, throughout the book and within other literature there are anonomous stories to the same extent. The book was made to tell the true stories of the women who had abortions; I believe that Sparrow would have done research before publishing the story to ensure it was true. The story is very accurate to the overall feel of abortions at that time; such as the shame and secrecy.
John Taylor’s Story
Mr John Taylor (1928-2008), consultant obstetrician and gynaecologist of Auckland, died on 30 December 2008. He was a key provider of services in Auckland for many years and was a respected teacher and trainer. He was interviewed in 2006.
The specialist I mostly worked with taught me a lot of obstetrics, which as a young GP I appreciated. He was great. He would come out any time I had a problem when a more experienced person may not have needed to call upon him. At the end of it he said, ‘You know you’re really enjoying this aren’t you?’ I said, ‘I have to be absolutely honest, yes I am’. He said, ‘Have you ever thought of going into O&G?’ I said, ‘I really have enjoyed this year and the training you’ve given me’. ‘Well, look’, he said ‘would you be interested in doing six months as a registrar in St Helen’s Hospital in Christchurch? You’d be working with some very fine people down there’. And I said, ‘Yes I think I would be interested. I think I could do that’.
So I went to Christchurch and I was a registrar at St Helen’s Hospital for six months. It was a wonderful six months. My career plans changed and I decided to go on with O&G. I was appointed as a house surgeon at National Women’s and then as a registrar before going overseas for further specialist training.
While at National Women’s there was one particular case that had a lasting impact on me. In October 1957 a lovely young lady was admitted to National Women’s Hospital where I was the registrar in the ‘C’ Team. She had been languishing in bed getting more and more ill, and came in with a high temperature of about 104 degrees. She had been too scared to present to anybody for medical help. As it transpired she had been to an illegal abortionist and the uterus had been only partially emptied of a 12 week pregnancy.
She was suffering from severe septicaemia to the extent that she had blood pressure collapse. We first had to attend to that, trying to sustain her blood pressure with noradrenalin drips. For the infection she was given massive doses of antibiotics. She had a lot of abdominal pain but for most of the time remained conscious. It reached the stage where the decision had to be made whether or not she should have a hysterectomy. This would have removed the cause of her septicaemia, the infected tissue in the uterus. However, the specialist in charge decided not to operate because her condition was so poor she would not have survived.
To make a long story short, after we had worked desperately with her for about 10 days, she died. As a team we had put so much time, effort and skill into trying to save her that her death came as a profound loss. I was severely affected by this tragedy, and I think it influenced the rest of my career in O&G.
We knew the social history and the circumstances surround her particular situation and what led to her having an abortion. They were just social pressures but pressures so strong that she felt desperate. Behind it all was the disgrace of having a baby out of wedlock. She couldn’t face up this this and didn’t want to disappoint her relatively conservative parents. We never found out where exactly she had been for the abortion. We left that to the police.
For this lovely young lady to lose her life in this way made me think there must be a better way. The numbers coming in with complications from illegal abortions were not huge. I suppose about one a month. When I say about one a month I’m only referring to one particular team. There were four teams, and they all had their own acute admissions. I didn’t like to pressure any patient so I never found out much about the illegal networks.
I was overseas for a year (1960) and then, having sat the exam in London, I was appointed registrar in the King’s College group of hospitals. I was then invited back to practise in Auckland and subsequently was appointed as a consultant at National Women’s. In my specialist training I learnt about abortion through clinical experience. I was exposed to septic abortion in England and there were other cases that reinforced my view but it was that one unforgettable case back in New Zealand in 1957 that turned it around for me.
With respect to my professional colleagues on the ‘C’ Team at National Women’s I suppose I felt more strongly than they did. Some of the senior consultants believed that if the grounds were mental health then you needed to get a psychiatric opinion to confirm that. That idea never appealed to me. I just thought it was a total farce to engage a fully qualified specialist psychiatrist on an abortion case. Our team only did abortions if there was a physiatrist who could say the women was likely to suffer severe depression.
Women had to go before a penal of three consultants, set up by the hospital to deal with requests for abortion. I remember when I’d only just been appointed as a very junior consultant forming part of a panel with two very senior gynaecologists. The other two said to me, ‘Of course there’s no way this woman will by psychiatrically affected. What do you think?’ and I said,’I just can’t agree with you I’m sorry’. They felt just as strongly as I did but in keeping with their own conservative views. I thought, ‘There’s got to be a better way. This is just untenable’.
At the panel the woman was interviewed in person; it was not just a matter of reading case notes. Consultations with the panel and the woman could take half an hour or so. After the consultation the panel conferred and made their decision. Then the woman wa brought back in to receive the decision in person. As far as my colleagues were concerned it was just open and shut. If she was a woman who was temperamentally normal in every other respect they could see no grounds for termination. At that time I suppose a strict interpretation of the law would be in accordance with their view.
I could ask specifically for a psychiatric report, but some of the psychiatrists were conservative bent, and they would agree with my conservative colleagues. One or two more liberal psychiatrist supported my professionally and would issue a report in favour of my opinion. But in general the whole scene was conservative because none of the senior gynaecologists were liberal at that time.
The ground of fetal abnormality raised different issues. Abortion was acceptable where there was a risk of a baby being born with a serious abnormality. The specialist had the surgical skills to undertake abortions, and I learnt surgical skills from them although I did very few as a registrar.
When I set up my specialist practice I included abortion services as part of women’s health care. It was not subjected to pressure from professional colleagues, even those with strong religious convictions. I always totally understood their situation and they mine. Increasingly colleagues came round to accepting the situation we had come to practise and at no stage did my views on abortion affect my professional development with regard to committees and jobs.
When the law changed, and the Auckland Hospital Board was required to provide an abortion service, I was invited down to a red carpet lunch, with hospital board cars provided, to meet Dr Fred Moody OBE, medical superintendent in chief. He said ‘John I want you to set up an abortion service for the Auckland Hospital Board.’ He had no doubt about wheat he was doing because he knew of my abortion views through my consultant colleagues. He wanted me to set up the Epsom Day Hospital and become its first medical director.
An earlier attempt to establish a day clinic by the Auckland Hospital Board had foundered. A licence was granted in May 1978 to St Margaret’s as part of the public hospital system. The previous owner, a doctor who did deliveries (and allegedly abortions), had left the premises to the Auckland Hospital Board. There was a huge fuss over the name because St Margaret is a Catholic saint who was killed for refusing to have sex with a Roman priest. She did a virgin and a martyr and became a patron saint of pregnant women.
Dr Peter Wilcox who previously worked as an operating doctor at AMAC, was appointed in June 1978, but resigned after his application to become a certifying consultant was refused by the ASC. Dr Wilcox’s case was raised in Parliament in July 1978 during the final debate on the amendments to the CS&A Act.
After my involvement in the Epsom Day hospital became known as SPUC used to protest outside our home when we had young children. It was pretty tough on the kids to have these banners and so on. My car used to be attacked, and graffitied, and tyres let down. They’d put stickers on the front and back windows – ‘Baby Killer’ – and all that kind of thing. One way and another I had quite a lot of contact with the SPUC people. I used to invite them to have a cup of morning tea. Our neighbours weren’t quite so happy. They used to turn the hoses on an inadvertently spray them. I didn’t find protest activity easy to take especially when it affected my wife and family. They kids had to cope at school, but I must say it didn’t stop my daughter studying medicine and becoming involved in abortion services.
I believe the law must allow for termination for a woman who finds herself profoundly desperate with an unplanned and unwanted pregnancy. I realise I may sound old fashioned and not in full accord with ALRANZ’s viewpoint, but I’ve always believed the present law isn’t too bad because it allows for termination on the grounds of mental health. I believe that if a women is forced to continue her unwanted pregnancy, then it is highly likely to adversely affect her psychological health to the extent that her health is endangered.
The present law is workable, and if you can judge things by the end results then it is very safe. There has not been a maternal death directly attributable to abortion since the new laws have been in place although the law cannot take the credit for that. The use of antibiotics to treat septic abortions was the most dramatic and life-saving advance. Furthermore the medical profession’s priority of saving lives as opposed to reporting crimes encouraged women to see medical treatment. The suction method using flexible cannulas was an improvement and could be carried out under local anaesthesia. Improvements in general anaesthesia made that safer when local anaesthesia was not an option. The use of ultrasound made the diagnosis of abnormalities and the estimation of gestational age more accurate. There were also improvements in blood transfusions, other intravenous fluids, and the treatment of pulmonary embolus (a risk after childbirth or abortion when a blood clot travels to the lungs). As well as these medical advances there has also been a general improvement in the nutrition and general health of the population.
The gain was not just in saving women’s lives but in protecting the health of the women. Unsafe abortions did not always kill, but could cause damage to the reproductive organs leaving a woman to suffer from painful complications or infertility, the inability to have children when they wanted to. I am convinced that total control over her fertility is a women’s right.
This story featured in the book Abortion Then and Now, a reliable and recognised book telling abortion stories during the Second Wave of Feminsim. http://alranz.wordpress.com/2013/07/12/history-and-dame-barbara-goodman/ backs up the story featuring in the book, it describes John Taylor and a brief description about his life and his job. As an author Margaret Sparrow, tells other peoples stories as quoted by them. However she has bias; she had an illegal abortion and heard stories later which lead her to write the book. Margaret Sparrow was one of the Family Plannings most well-known doctors, after she attended a Family Planning Association conference she continued to exceed to give women options such as contraception.
